
Over the past 25 years, Have Dummy Will Travel has trained tens of thousands of people in CPR and AED use. Over the years, we’ve had a handful of folks call to thank us– that the skills they learned were used to save someone’s life. Very rarely do we get the opportunity to download the code summary data from the AED, reconstruct the event, and dissect it to learn what we can do to improve performance and patient outcomes. Such an event occurred recently in one of our client’s dental offices. With permission of the client, I offer the following expert analysis.
Case Review
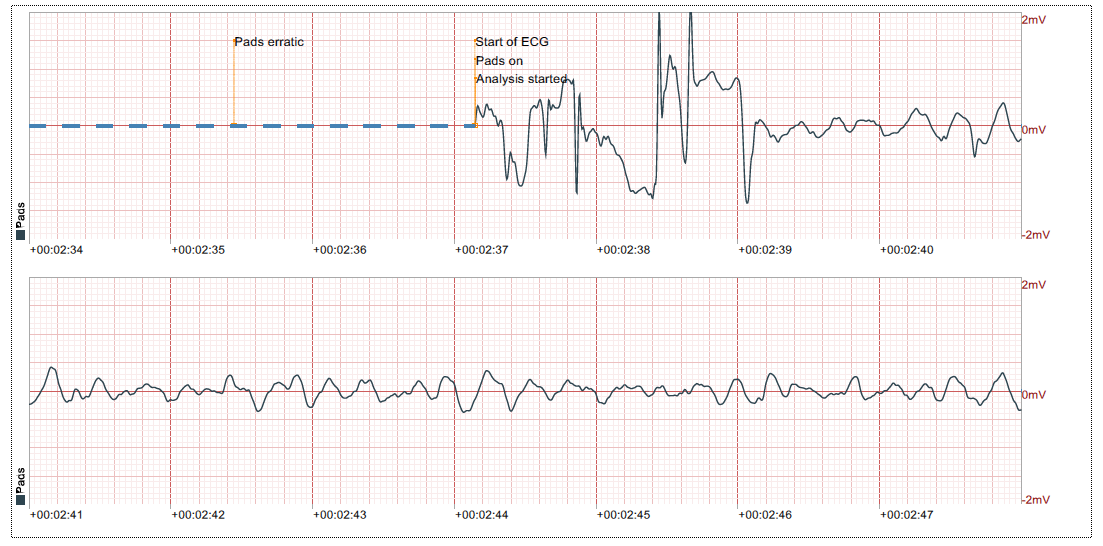
The patient was an 83 year-old male who went into cardiac arrest during a dental procedure. The dentist immediately removed the rubber dam and began chest compressions while the patient was still in the dental chair. The assistant activated 911 and retrieved the Philips Heartstart AED. Upon arrival of the AED, it was turned on, and as we can see from the ECG, the pads were eventually placed on the chest, about two and a half minutes later. According to the client, the delay occurred because, in the heat of the moment, he hadn’t realized that the plastic liner was still on the pads. Despite the delay, the initial rhythm (below) is coarse ventricular fibrillation (VF), indicating that high quality CPR was being administered in the interim.
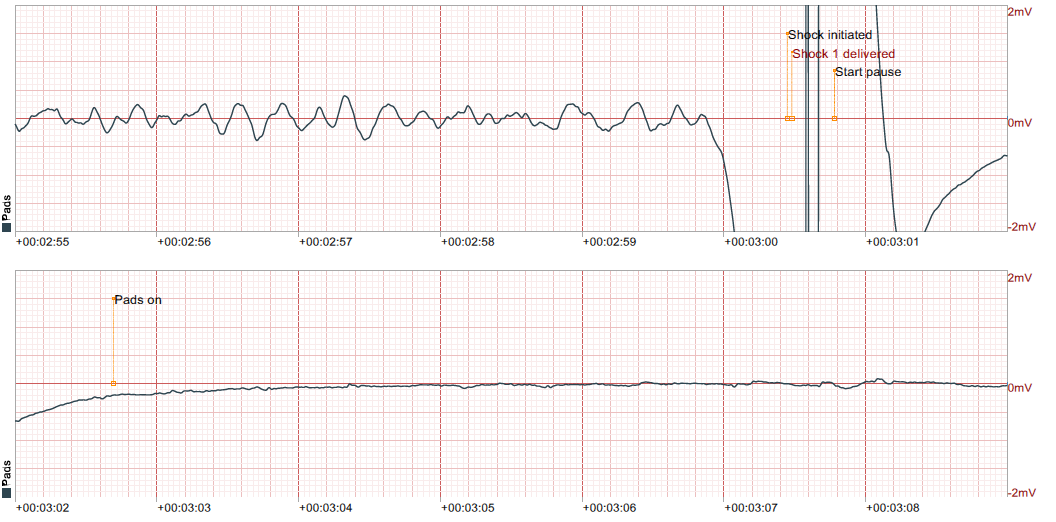
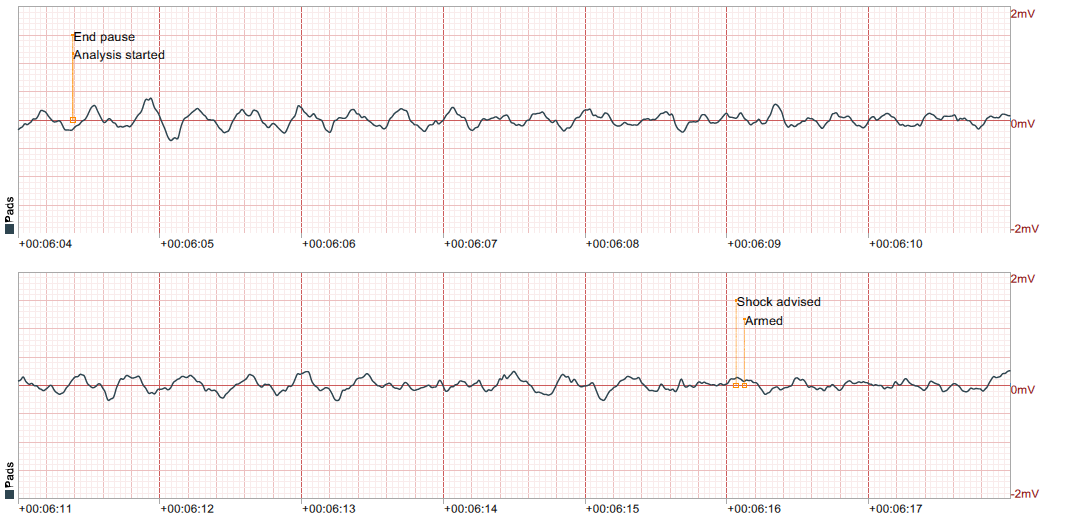
High-quality CPR includes pausing compressions for no more than 10 seconds. For this reason, AEDs are programmed to analyze and be ready to shock within 10 seconds During this time, no CPR is supposed to be occurring so that the AED can analyze. Note the time of shock in the ECG above. Twenty-three seconds elapsed between the initial analysis and delivery of the shock.
The ECG above also shows that the shock changed the rhythm to asystole. Evidence of chest compressions resuming can be seen below– 16 seconds after the shock, despite AED voice prompts instructing the user to begin compressions again. Therefore, total of about 40 seconds went by without compressions.
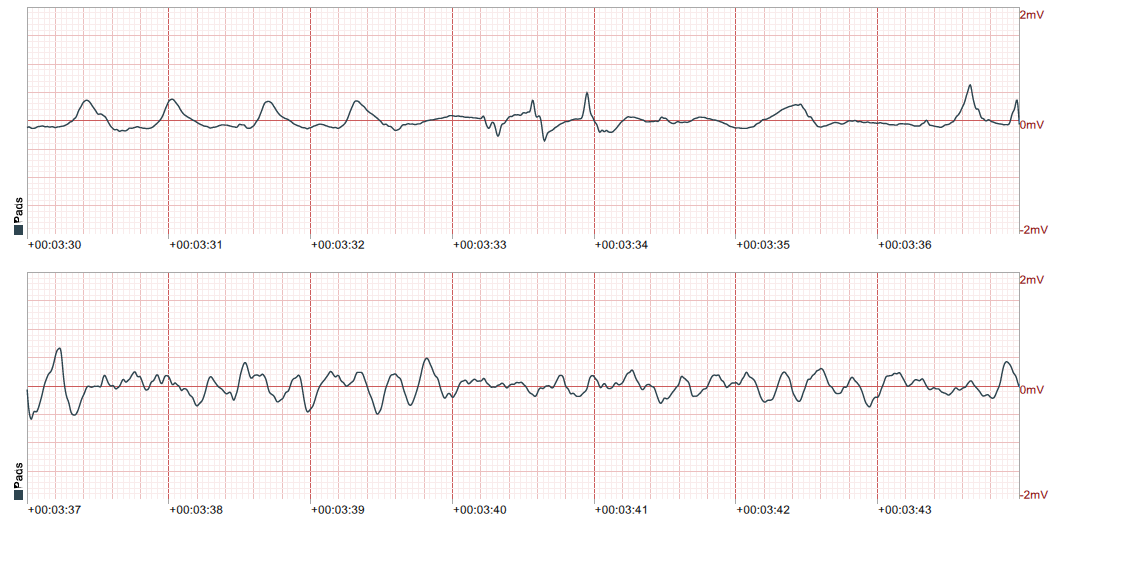
According to Philips, the AED is set to coach rescuers to give compressions at a rate of 100 / min. This is the lower end of the current Emergency Cardiac Care (ECC) guidelines target of 100 – 120 / min. The ECG below is consistent with this..
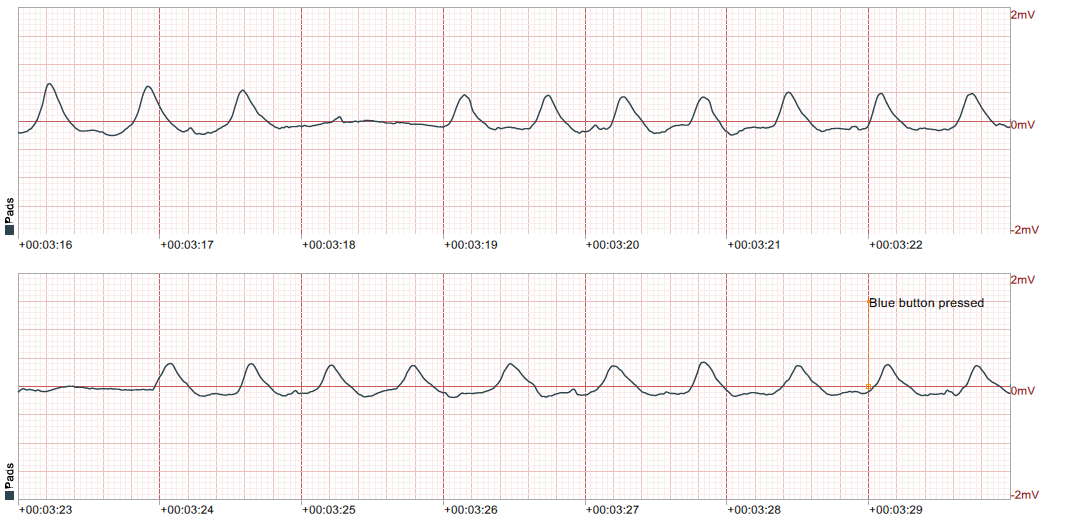
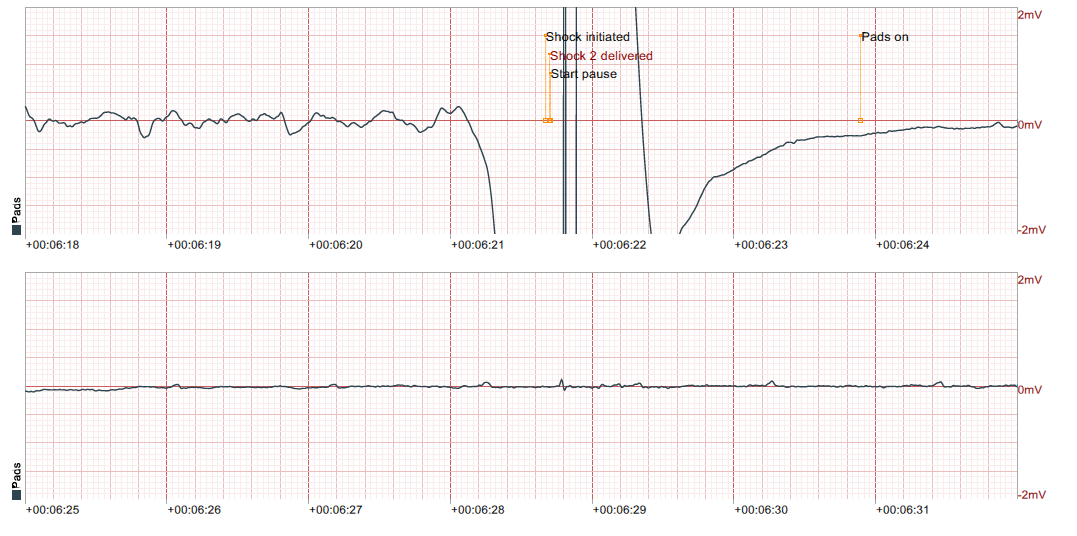
The ECG below shows the moment when the dentist stopped CPR and handed the emergency over to a police officer. The patient was lowered to the floor and poor quality CPR resumed for the next three minutes. It is important to note that prior to this moment, the underlying rhythm had changed back to ventricular fibrillation (VF), after just about 20 seconds of chest compressions, indicating the dentist was doing a great job at giving high-quality CPR. Also note that after handing off the emergency to the police officer, the amplitude of the waveform flattens as time continues, indicating the quality of CPR is diminishing, if being performed at all. Without blood flow to the heart muscle itself, the energy and oxygen reserves in the heart are quickly depleting, and anaerobic respiration is beginning to be the dominant form of ATP production. Without oxygen infusion into the cells, this rhythm will eventually become a flat line, also known as asystole. This is precisely what occurred after the next shock, as seen at time 6:21, below.
Another important note to make is that although the AED is programmed to reanalyze the ECG and reevaluate for a shockable rhythm after 2 minutes, it did not do so for 3 minutes after the first shock. In talking with Philips USA’s tech team, I learned that the 2-minute counter begins after the AED gives instructions to begin compressions and sounds the metronome. In this event, the blue “i” button was pushed at 3 minutes 29 seconds (not shown here). This causes the internal timer to reset, and a set of verbal instructions to be given to the rescuers. Pushing the “i” button in the melee delayed the time to next analysis and shock.
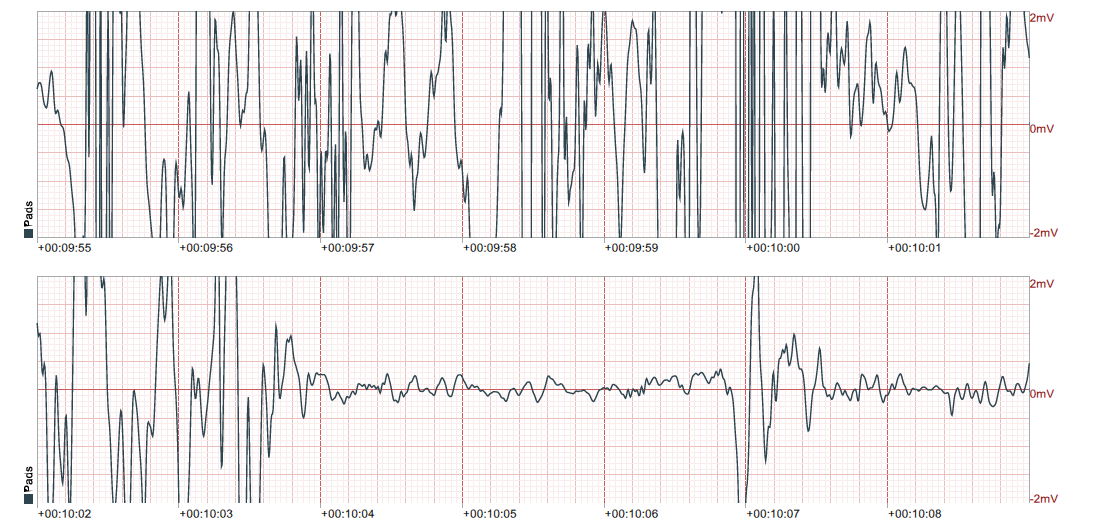
Upon arrival of EMS, a “Lucas” device was applied to the patient. This device provides perfect chest compressions, tirelessly. You can see the difference in the ECG below. Note that only about 10 seconds of Lucas device compressions returns the rhythm to VF, as the device was paused so it could be adjusted on the patient’s chest.
The story ends less bleak. With two additional shocks, epinephrine and a couple of doses of antiarrhythmic medication, the return of spontaneous circulation (ROSC) was achieved. Two weeks later, the patient was extubated in the ICU with normal brain function, but could not move his extremities and had acute kidney injury. His current disposition is not known.
Analysis
So why do we see what we do on the code summary? To demonstrate, hold up a large textbook or similar item in one hand, suspending your arm above any surface. Keep the item held up as long as you can. What are you feeling in your arm as you hold the object up? Most folks will say that their arm gets tired, feels weak, or perhaps has a burning sensation.
In order to keep the load suspended, the muscles in your shoulder need to twitch, or contract. Contraction requires energy, both to slide the filaments of the muscle cells past each other, causing them to get shorter, but also to reset them to a resting stage, so they can contract again later. Energy comes in the form of Adenosine Triphosphate (ATP) molecules that are, for the most part, produced in the mitochondria of the cells.
During contraction, the first few seconds worth of ATP molecules comes from excess, resident ATP that is waiting to be used. The next 20 seconds comes from the transfer of a phosphate group from creatine phosphate to ADP– a very quick process called direct phosphorylation. But this source exhausts quickly as there is a finite amount of creatine phosphate available. The greatest amount of ATP is produced through aerobic respiration.
The first step, glycolysis, occurs outside the mitochondria of the cell. One molecule of glucose yields 2 ATP molecules plus pyruvic acid. The pyruvic acid moves into the mitochondria and in the presence of oxygen, undergoes the series of Krebs cycle reactions, to form another 34 ATP molecules. Aerobic respiration yields a total of 36 ATP for every single glucose molecule used.
As you were trying to hold the book up you needed more ATP than you could produce, because oxygen was quickly depleted from the muscle cell, and became a limiting factor. Your circulatory system could not get enough oxygen to the muscle cells quickly enough to produce sufficient amounts of ATP. Therefore, you were producing an abundance of pyruvic acid in glycolysis, but now the pyruvic acid was fermenting into lactic acid in the process of anaerobic respiration. If you did not put the book down, you would have dropped it– the muscle would have eventually failed. Did you feel the burning sensation of lactic acid flushing out of the muscle the moment you put that book down?
Below is a looped video showing the heart in VF. Note that the muscle is twitching, just not in any organized fashion, and so it is ineffective in pumping blood forward to perfuse the organs of the body, including itself. Twitching, even when chaotic, requires energy. While there may be adequate glucose reserves in the muscle cell, oxygen is depleted, and so ATP cannot be produced with great efficiency. The muscle fills with lactic acid. The shock from the AED causes every cell to depolarize simultaneously, in hopes of resetting the cardiac cycle, allowing the sinoatrial node to again become the pacemaker, returning the heart rhythm to one that is perfusing. Without energy, the muscle cannot twitch and the nervous tissue cannot depolarize. Therefore repolarization of the cells does not occur, and asystole or pulseless electrical activity (PEA) ensues.
High quality chest compressions is the only way a lay rescuer can help deliver the resources needed to produce an overabundance of ATP. Eventually, if all goes well, the combination of chest compressions, medications, and defibrillatory shocks will bring about ROSC, as the EMS crew did. Immediate, high quality chest compressions both before AND after a defibrillation shock is what saves lives.
As heart muscle dies from lack of nutrients and oxygen, rhabdomyolysis ensues. The cell membranes break down and release myoglobin protein into the bloodstream. These proteins affect the kidneys, effectively clogging the nephrons, resulting in acute kidney injury (AKI). Much of the damage done in AKI may be irreversible, and even a patient who is successfully resuscitated may later die due to low kidney function and toxin buildup.
Lessons Learned
- Practice does make perfect.
When humans are encountered with tremendous stress, such as this emergency, we react in one of three ways: flight, fight, or freeze. These are not conscious decisions, and are controlled solely by our sympathetic nervous system. For this reason soldiers and police officers are taught tactical breathing and other ways to “get off their X”, which marks the spot they are frozen on. One of the effects of the sympathetic nervous system is tunnel vision. The ability to see the bigger picture is dampened and something like not realizing the liner on the pad hadn’t yet been removed happens. I often see this same type of “deer-in-headlights” response when I field-train new EMTs and paramedics experiencing their first serious case. I may have even had the same type of experience myself almost 30 years ago. Only through practice and frequent drills could a minor detail like that have been seen and corrected immediately. The lesson: Make sure you and your entire team are keeping up with your CPR AED recertifications. Additional drills a few times per year (something Have Dummy Will Travel can help you with) are also helpful so that when the real thing occurs, you have been desensitized enough that the event becomes “just another day in the office”.
- Immediate, high quality chest compressions (and defibrillation) is of paramount importance.
As described above, delivering chest compressions both before and after defibrillation saved this patient’s life. If you are alone and witness cardiac arrest, grab the AED and apply it immediately. If you have a team around you, start CPR while someone else retrieves the AED for you. If you did not witness the arrest, perform chest compressions for two minutes before applying the AED quickly.
- Review the technology in your AED.
Any AED that was purchased around 2012, when the law requiring dentists to have an AED came about, has an expired warranty. The technology in these devices is 40 years old, with little improvement. The software in the Philips device, for example, does not pause to let the user know that the unit is charging. During this charge phase of about 5-8 seconds, an opportunity to continue high-quality compressions is missed.
In addition, Philips delivers the same amount of energy to every patient, regardless of patient size or amplitude of VF. A newer unit might measure the patient’s BMI and the amplitude of the VF, and will customize the energy to be delivered. The energy level in subsequent shocks will be escalated automatically. Newer units can also recognize supraventricular tachycardia and treat it with synchronized cardioversion.
The shock from a semi-automatic defibrillator requires the user to push the shock button. This can be very intimidating, and it may take a few seconds to build up the courage to push the button. We see this very often in both training scenarios, and out in the field. In a cardiac arrest, seconds count, and may be the difference between life and death. Newer AEDs are available as fully automatic, removing the hesitation to deliver the shock.
If you have an older AED, it might be time to replace it with upgraded technology. Have Dummy Will Travel can help you make such decisions.
- Resume chest compressions immediately after the shock is delivered.
The time over which the shock is delivered is nanoseconds. People are not batteries, we do not store a charge. Therefore, chest compressions can, and should be, resumed immediately after the shock is delivered. You do not need to wait for the AED to tell you it is safe to touch the patient. To reduce the amount of hands-off time even further, advanced providers are taught to “hover” over the patient, ready to deliver compressions during analysis and the actual shock delivery time.
- Do not use the rescue coach.
AEDs have built-in rescue coaches to help get the rescuer through the emergency. They are designed to talk anyone through the procedure of applying the AED and delivering a shock, even if that person has never taken a CPR AED class before. As an aside, New York State public access defibrillation law does not allow anyone who is not certified in CPR AED to use an AED.
We train every healthcare provider NOT to use the rescue coach unless you need it to “get off your X” (see above). If you know what you are doing, the rescue coach will only hinder your progress. As we saw in the case study, summoning the rescue coach delayed the second shock to the patient, when he was not receiving high quality chest compressions. This increased the amount of lactic acid in the heart muscle, while depleting ATP and ATP-producing resources.
- Effective compressions CAN be done in the dental chair.
We have the evidence that compressions that were performed in a dental chair were at least somewhat effective. To drag an unresponsive adult human from a chair to the floor, and then to a space in the office that is wide-open enough to work takes time, and can potentially cause the rescuer to incur back injury.
A dental chair offers the added feature of lifting the patient up or lowering him/her down, adjusting for the height of the rescuer, supporting effective compressions to be administered by almost anyone. For best results, and to ensure the compressions do not cause damage to your chair, I suggest sliding the patient down the chair so that the middle of the chest is close to the seat, where the greatest support would be. Position the top of the chair all the way back to support opening the patient’s airway.
- Regardless of where you are, be prepared to work the code for several minutes.
One of the most common comments I hear from clients is that “the fire department is right down the road”. In this case study, the ambulance was located only one mile away from the dental office and was fully staffed at the time they were alerted. Still, paramedics were not on scene for over 9 minutes. Depending on where you are, a fully staffed ambulance may not be waiting for you to call. You may need to wait additional time for volunteers to leave their homes and drive to the ambulance garage, gear up, and then drive to you. Additional time is taken up in relaying the message from the 9-1-1 call taker to another dispatcher who activates the ambulance response.
In high-quality CPR, compressors switch every two minutes while the AED analyzes. In the above scenario, the patient should have received four shocks and four different compressor switches BEFORE paramedics arrived. If your entire team is not trained and ready to pitch in, the quality of any single person’s compressions will dwindle, as will your patient’s chances of survival.
- Even when EMS arrives, you’re in it for the long haul.
In this case, EMS worked the patient for about 20 minutes until they achieved ROSC, and deemed the patient stable enough for transport. This is pretty standard for cardiac arrests, and may even go longer. In that time, you can only stand back and give paramedics any information you have regarding the patient’s medical history, medications and allergies. Please don’t push them to work faster, or to take the patient out of the office. At that point, paramedics are the best chance the patient has, but you need to let them work.
Erik Zalewski is a Nationally Registered Paramedic and New York State EMS Certified Instructor Coordinator with over 28 years experience responding to 9-1-1 calls for medical emergencies. Erik has taught EMTs and paramedics at Stony Brook University, Borough of Manhattan Community College, and the Suffolk County, NY EMS academy. He and his team at Have Dummy Will Travel, Inc. are dedicated to helping medical professionals respond to emergencies safely, efficiently and in the most cost-effective manner possible. Call or text 631-849-4978 for additional information.